
Nerve compression injuries are a common cause of pain and discomfort. When there are multiple locations of compression on a nerve it is called a double or multiple crush injury. A common double crush combination involves symptoms of thoracic outlet syndrome existing along with those of carpal tunnel syndrome. Double crush can occur in the lower extremity as well. Sciatic nerve compression by the piriformis muscle could exist along with nerve compression in the posterior thigh or tarsal tunnel in the ankle. It important to recognize when a double crush injury might be present because treatment needs to focus on multiple locations to be effective.
To better understand double crush injuries, let’s look at some nerve physiology first. The section of nerve closest to the spinal cord is called the nerve root (Figure 1). There is a dorsal root that contains sensory fibers going into the spinal cord and a ventral root with motor fibers leaving the spinal cord and supplying peripheral muscles. Fibers from the sensory and motor roots then combine to become the nerve trunk. Multiple nerve trunks join together as they leave the spinal cord on their way to the extremities.
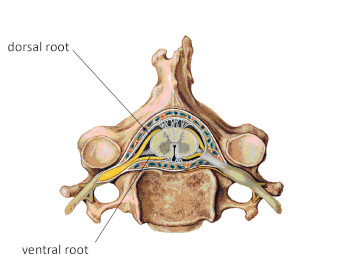
Figure 1
Nerve roots as they exit the spine
Mediclip image copyright (1998) Williams & Wilkins. All Rights Reserved.
Bundled together, these nerve trunks make up a group of nerves called a plexus. A good example is the brachial plexus in the cervical region. A plexus often has numerous connections between the different trunks (Figure 2). As the nerve trunks leave the plexus, they separate into distinct nerves that supply different regions of the extremities. Each of these separate nerves is called a peripheral nerve. The median, radial, and ulnar nerves of the upper extremity are examples of peripheral nerves.
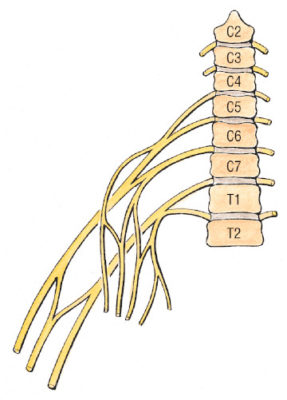
Figure 2
Schematic representation of the brachial plexus
Mediclip image copyright (1998) Williams & Wilkins. All Rights Reserved.
There are different names for nerve compression pathologies depending on where the compression occurs along the nerve’s path. Adverse pressure on a nerve root is called a radiculopathy. Adverse pressure applied farther along a peripheral nerve is called a neuropathy. Sometimes pressure on a nerve trunk where it is still part of a plexus may be called a plexopathy.
Once the nerves exit the spinal cord, they are surrounded by several connective tissue layers, including the endoneurium which surrounds each nerve fiber. The nerve fibers collect in bundles called fascicles that are surrounded by another connective tissue layer called the perineurium. Numerous bundles of fasicles then make up a peripheral nerve, which is enclosed within another connective tissue layer called the epineurium (Figure 3). These layers of neural connective tissue play an essential role in nerve compression pathologies like the double crush.
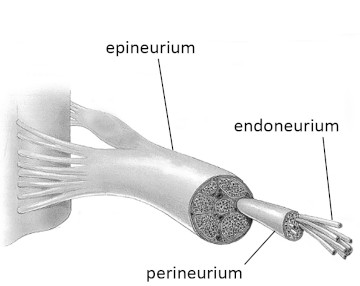
Figure 3
Divisions and connective tissue layers of a peripheral nerve
In addition to the connective tissue layers and nerve fibers contained within a peripheral nerve, there is an intricate vascular supply to each nerve as well. This vascular network consists of tiny vessels within the nerve that supply the blood flow essential for the nerve’s proper function. Ischemia (lack of blood flow) due to compression is likely to cause neurological symptoms and plays a role in the double crush syndrome as well.
The connective tissue layers also serve as a tube for the transmission of cellular fluids. The nerve carries its own nutrient supply that is necessary for proper function. The nutrients are moved along through the nerve by a slow-flowing cytoplasm within the nerve cell called axoplasm. The flow of axoplasm inside the nerve fiber is called the axoplasmic flow. If there is a disturbance to this flow (often caused by nerve compression), the individual may experience neurological symptoms such as pain, paresthesia, numbness, or motor impairment.
The double crush happens because a blockage in axoplasmic flow in one region may impair the function of tissues in distant regions of the nerve. For example, if a person has a proximal compression on the brachial plexus, everything distal to that site is more susceptible to pathology because there is a blockage in the axoplasmic flow and, therefore, a deprivation of nutritional supply to the distal nerve tissues. The double crush could be a reason why so many clients appear to have simultaneous symptoms of thoracic outlet and carpal tunnel syndromes. While this condition is often called the double crush phenomenon (or syndrome), there may be more than two sites of compression on the nerve. In this case, the problem would be considered a multiple crush injury.
One of the critical problems with many approaches to treating nerve compression problems in the extremities is viewing the problem as an isolated compression in only one location. For example, if a person has median nerve pain in the hand there may be an assumption that the problem is limited to compression in the carpal tunnel. Consequently treatment is usually aimed only at the region of the carpal tunnel.
One of the distinct advantages of massage treatment for nerve compression disorders is the integrated wholistic approach that most massage treatments include. Rarely would a massage treatment only work on the wrist without also addressing the entire upper extremity, shoulder, and neck regions as well. This more comprehensive approach to treatment makes massage an excellent strategy for addressing multiple crush nerve injuries.
The massage therapist is most effective when adequately addressing tissues along the pathway of the affected nerve. Consequently, you need to know the anatomical path of the primary peripheral nerves and also be familiar with some common locations where nerve compression is likely to occur. That way you can adequately address those regions with a variety of approaches that will have the highest chance of reducing any compression or binding of the nerve.
If your client is presenting with peripheral nerve compression symptoms, be sure to consider the possibility of multiple crush and treat the entire nerve pathway thoroughly. Failure to provide a comprehensive treatment of the full nerve pathway could result in frequent recurrence of the problem and potential long-term nerve impairment.